Friday, 30 June 2023
Wednesday, 28 June 2023
Wednesday, 21 June 2023
The Anatomy of the Brainstem

Friday, 16 June 2023
3D printing of brain blood vessels could revolutionise neurosurgery–new technique shows how

Thursday, 15 June 2023
Suprascapular Nerve Block
What are the Indications of the Suprascapular Nerve Block?
A suprascapular nerve block may be recommended for the treatment of:Acute pain from a shoulder injury
- Pain following shoulder surgery
- Adhesive capsulitis also called frozen shoulder
- Rotator cuff injuries
- Arthritis
- Bursitisand cancer pain
- Prior to the Procedure

Following the procedure, your shoulder will feel numb for a short time from the local anesthetic. The pain may return once the anesthetic wears off and you may feel soreness at the injection site.
The steroid can take up to 2 weeks to begin working and provide pain relief that can last a few weeks to a few months. Sometimes the medication does not provide any relief at all and will depend on the person.Avoid driving yourself home if you have received sedation for the procedure.
Avoid straining the shoulder for at least 24 hours after your procedure.
Any swelling at the site of injection may be treated by applying ice to the area.
What are the Risks and Complications of Suprascapular Nerve Block?
Although suprascapular nerve block is a relatively safe procedure, it may be associated with complications such as:Bleeding or infection at the injection site
- Nerve injury
- Pneumothorax
- Allergic reaction
Tuesday, 13 June 2023
Need a mental health day but worried about admitting it? You’re not alone
There are days when it’s hard to face work, even when you aren’t physically sick. Should you take a day off for your mental health? If you do, should you be honest about it when informing your manager?
If you work for an organisation or in a team where you feel safe to discuss mental health challenges, you are fortunate.
Despite all the progress made in understanding and talking about mental health, stigma and prejudices are still prevalent enough to prevent many of us from willingly letting bosses and coworkers know when we are struggling.
Mental health challenges come in different forms. For some it will be a severe lifelong struggle. For many others the challenge will be periods of feeling overwhelmed by stress and needing a break.

Globally, the World Health Organisation estimates about 970 million people – about one in eight people – is suffering a mental disorder at any time, with anxiety-related disorders affecting about 380 million and depression about 360 million.
These numbers have jumped about 25% since 2019, a rise credited to the social isolation, economic hardship, health concerns and relationship strains associated with the pandemic.
But declining mental health is a longer-term trend, and it’s likely work demands have also played a role. Research identifies three main workplace contributors to mental ill-health: imbalanced job design when people have high job demand yet low job control, occupational uncertainty, and lack of value and respect.
This at least partly explains why depression and anxiety appear to be more prevalent in wealthy industrialised nations. In the United States, for example, it is estimated more than half of the population will experience a diagnosable mental disorder at some point during their lifetime.
Visit: neurology.pencis.com
#MentalHealth#MentalWellness#MentalHealthMatters#EndTheStigma#BreakTheStigma#MentalHealthAwareness#MentalHealthSupport#MentalHealthWarrior#SelfCare#SelfLove#SelfCompassion#MentalHealthAdvocate#YouAreNotAlone#Mindfulness#PositiveMentalHealth#MentalHealthRecovery#AnxietyAwareness#DepressionAwareness#BipolarDisorder#PTSDAwareness#SuicidePrevention#EndSuicide#MentalHealthFirstAid#Wellbeing#TherapyWorks#MentalHealthResources#MentalHealthEducation#MentalHealthMovement#EmotionalWellness#MindOverMatter
Monday, 12 June 2023
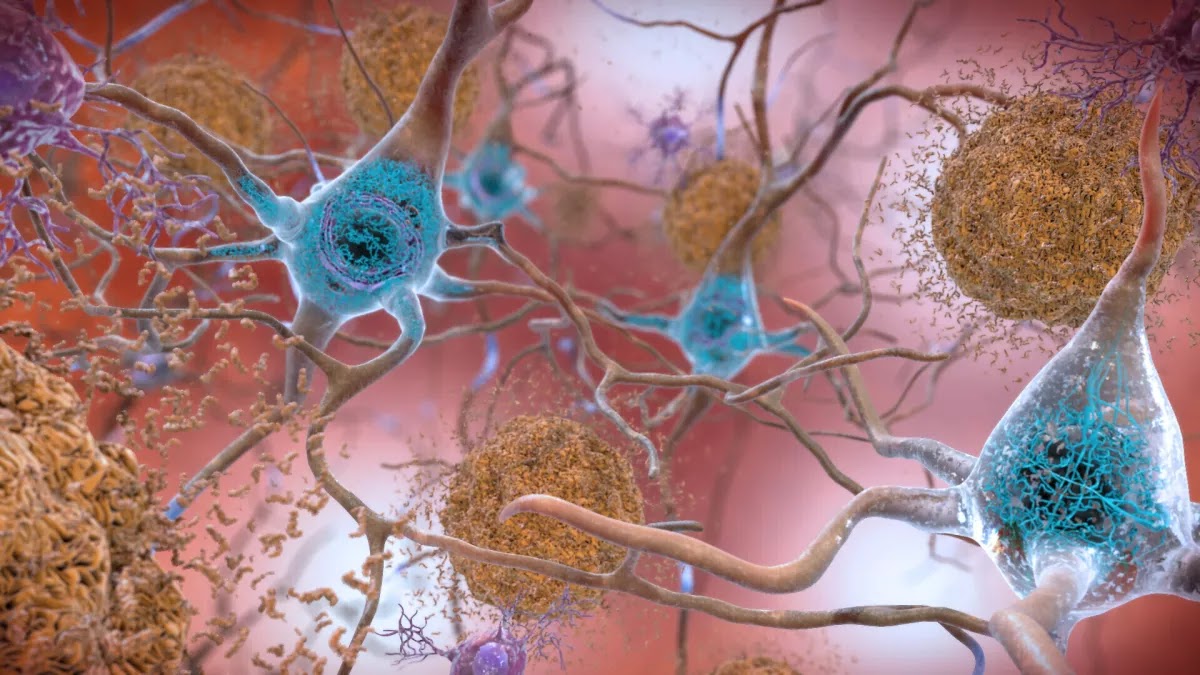
Opinion: New Alzheimer’s drugs are costly and controversial. Are we going about this all wrong?
Saturday, 10 June 2023
Friday, 9 June 2023
Research sheds new light on the genetic architecture of bipolar disorder

Visit: neurology.pencis.com
Wednesday, 7 June 2023
Saturday, 3 June 2023
Pediatric Neurology Devices Market expected to reach a value of USD 3.26 billion by 2029. The market is anticipated to grow at a CAGR of 6.3% during the forecast period.
• Global Market, by Product (2021-2029)
• Global Market, by Service (2021-2029)
• Global Market, by Application (2021-2029)
• Global Market, by Neurological Subspecialties (2021-2029)
2. Regional Pediatric Neurology Devices Market (2021-2029)
• Regional Market, by Product (2021-2029)
• Regional Market, by Service (2021-2029)
• Regional Market, by Application (2021-2029)
• Regional Market, by Neurological Subspecialties (2021-2029)
• Regional Market, by Country (2021-2029)
3. Company Profile: Key players
• Company Overview
• Financial Overview
• Global Presence
• Capacity Portfolio
• Business Strategy
• Recent Developments
